

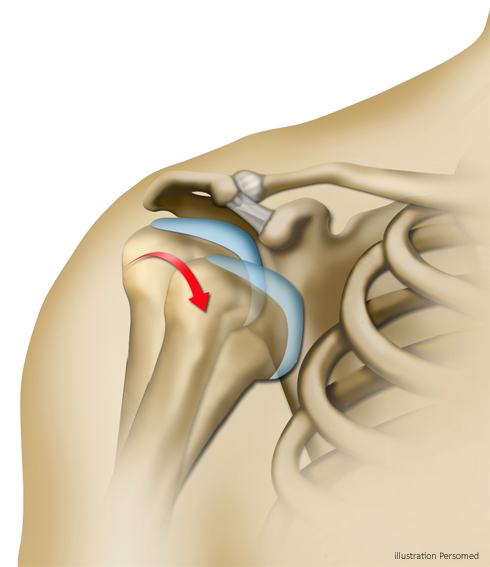
In the shoulder joint, the contact surface between the humeral head and the glenoid of the scapula is quite small. It is not a completely nested joint, like the hip for example, and its stability is largely ensured by the articular capsule.
We speak of dislocation when the humeral head comes out completely, or of subluxation when it comes out partially. When these phenomena are repeated, we speak of shoulder instability.
In the vast majority of cases, the first dislocation is due to a major trauma (fall, rugby tackle, etc.), and then the following episodes of instability will occur during less violent trauma or movements. In people with particularly flexible joints, we speak of congenital hyperlaxity.
Each episode of instability can result in lesions on the glenoid rim, labrum or capsule. These elements, which often do not heal properly, will no longer be able to ensure the stability of the shoulder.

Your surgeon will need an X-ray to evaluate bone lesions and an CT arthrography to visualize lesions on tissue and cartilage.
Below, an animation to better understand the mechanism of shoulder instability (in French)
Treatment options
Medical Treatment
Initial form of management for shoulder instability is rehabilitation, which is essential for strengthening muscles that stabilize the shoulder.
Surgical Treatment
If rehabilitation is not enough, stabilization surgery should be considered. Age and physical activity are decisive factors in the decision of surgery.
At the Bordeaux-Merignac Sport Clinic shoulder specialists surgeons perform a procedure combining two techniques : the Latarjet and Bony Bankart.
